Definition
Cataract is the clouding of normal crystalline lens of the eye. It develops slowly and results in gradual progressive decrease in vision. It may affect one or both eyes.
Causes
1. Age related cataract. Seen in patients more than 60 years of age.
2. Congenital or developmental seen in children with TORCH infections, Marfans and other syndromes
3. Traumatic and foreign body injury.
4. Metabolic like calcium, phosphorus deficiency.
5. Exposure to radiation.
6. Drugs like steroids
7. Associated with systemic diseases
8. Eye Condition such as uveitis and high myopia (numbers more than – 6)
How to know that you have cataract?
1. Decrease in vision for near, distance or both
2. Glare (Trouble with bright lights)
3. Halos (Seeing rings or colors around bright lights)
4. Decreased night vision
5. Decreased contrast sensitivity
6. Decreased ability to recognize colours.
Types of Age Related Cataract
1. Nuclear sclerotic
2. Cortical
3. Posterior Subcapsular Cataract
Diagnosing Cataract
Your ophthalmologist can diagnose it using simple OPD tests and procedures.
1. History of previous illness and medication
2. Visual complaints
3. Visual Acuity testing
4. Visual field testing
5. Slit Lamp examination
6. Dilated examination
7. Specular microscopy
8. IOL power calculation
When should you have cataract surgery
Your Ophthalmologist will not advise surgery unless the cataract interferes with your daily activities or prevent you from leading a productive life. The only treatment for cataract, however, is surgical removal of cataract. A cataract does not have to become “ripe” before it can be removed. With modern advances in cataract surgery, the lens can now be removed from the eye at any stage of development.
It is true that the longer a cataract develops, the more it hardens. At advanced stages, a firmer or more developed cataract can be difficult to remove.
It is also true that if cataracts are allowed to develop for long periods of time, they can cause inflammation or increased intraocular (within the eye) pressure that can lead to glaucoma.
It is therefore safer to remove a cataract sooner rather than later. Phacoemulsification gives better results in most of the cases.
Treatment
Treatment consists of surgical removal of the cataract (opaque natural lens in eye) and replacing it with an intraocular implant (lens).
Anaesthesia for Cataract Surgery
1. Peribulbar injection
2. Subtenons injection
3. Topical with anaesthetic drops and/or jelly
The main advantage of topical anaesthesia is reduced hospital stay. There is no added advantage in terms of visual outcome. Topical anaesthesia requires careful patient selection and counselling by the surgeon.
Techniques of surgery
1. Phacoemulsification-
- It is the most widely used method for cataract extraction currently.
- It is performed through a 2-3mm incision.
- In this technique ultrasound waves are used to emulsify the cataract through a small opening in the anterior capsule using a hand held probe.
- The emulsified cataract is then aspirated.
- An artificial implant usually made of acrylic material is the placed inside the capsular bag.
2. Small Incision Cataract Surgery-
- In this technique the cataract is manually extracted through a 5-6mm incision which is self-sealing and does not require suturing.
- A PMMA or Acrylic implant is then placed inside the capsular bag.
- This technique is generally preferred in cases of hard cataract or where phacoemulsification is not possible
3. Extracapsular Cataract Extraction (ECCE)
- Older Method
- Cataract is extracted through a large 10-12mm wound
- Stitches are taken to close the wound
- May be required in certain cases like hard cataract or traumatic cataracts
| PHACO | Small incision cataract surgery | |
|---|---|---|
| INCISION | 2-3mm | 5-6 mm |
| ANAESTHESIA | LOCAL INJECTION/TOPICAL | LOCAL INJECTION |
| TYPE OF LENS | FOLDABLE | RIGID |
| RECOVERY | 1-2 WEEKS | 3-4 WEEKS |
| HOSPITAL STAY | DAYCARE | DAYCARE |
Choice of Surgery
Depends upon
1. Type and grade of cataract
2. Age and endothelial count of patient
3. Associated eye conditions
4. Financial condition of patient
Different types of Intraocular Implants(Lenses)
1. Non foldable lens-rigid lens made up of PMMA
2. Foldable Lenses
- Monofocal
- Toric(for higher preoperative astigmatism)
- Trifocal
- Multifocal
Which lens is suitable for me
1. Lifestyle and activities of patient
2. Age of patient
3. Associated medical and ocular conditions
4. Visual outcome expectations of patient
5. Financial condition of patient
Dos and Dont’s after Cataract Surgery
1. During the first week after surgery, it generally is recommended that the patient keep his or her eye covered at all times, either with eyeglasses or an eye shield, to protect it from being bumped or rubbed.
2. Patient is required to instill drops in the operated eye as advised
3. Patient id require to continued his systemic medication as advised by physician
4. Patient is required to avoid the following
- Bending over
- Lifting weights more than 5kg
- Rubbing the eye
- Splash water onto the face
- Straining for motions or passing urine
Complications of cataract surgery
They are very rare with newer techniques. Hence all instructions should be followed as given by your doctor.
1. Corneal oedema
2. Posterior capsular rupture
3. Nucleus drop(a part or entire cataract drops into back of eye
4. Infection(Endophthalmitis)
5. Retinal detachment
6. Cystoid macular oedema
7. Posterior capsular opacification(Late)
DIABETES MELLITUS AND THE EYE
Diabetes Mellitus is a metabolic disorder characterized by presence of hyperglycemia (increased blood sugar) due to defective insulin secretion, defective insulin action or both. This leads to chronic hyperglycemia which causes specific long term microvascular complications. Diabetes mainly affects the eyes, the kidneys, the nerves and the cardiovascular system.

Complications in the eye
1. Diabetic retinopathy
2. Cranial Nerve palsy
3. Optic Neuropathy
4. Cataract
5. Secondary neovascular Glaucoma
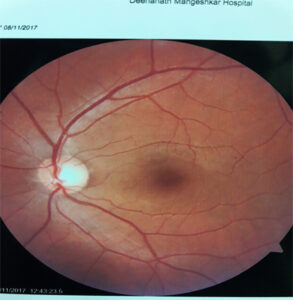
Diabetic retinopathy
A highly specific retinal microangiopathy occurring in both type I & Type II Diabetes mellitus
It is the most common cause of legal blindness in working adults
Patient may have normal vision in spite of extensive changes in the retina.
It is preventable. Risk of blindness is 10-15 times more in diabetic patients as compared to non-diabetics
Risk factors for developing diabetic retinopathy
1. Duration of Diabetes
2. Poor control of blood sugar
3. Associated hypertension and renal disease
4. Pregnancy
5. Hyperlipidemia
6. Obesity
7. Smoking
8. Cataract surgery
Pathology
Diabetic retinopathy is a microangiopathy in which there is cellular damage which mainly affects small blood vessels which results in capillary dysfunction. Capillary non-perfusion leads to retinal hypoxia which results in formation of new vessels as a result of increased vascular endothelial growth factor(VEGF).
Retinal Changes seen in Diabetic retinopathy
1. Microaneurysms
2. Retinal haemorrhages
3. Exudates
4. Cotton wool spots
5. Venous changes
6. Intraretinal microvascular abnormalities
7. Macular edema
8. New vessel formation on disc, elsewhere on retina or iris
Modified Airlie House Classification and International Clinical Disease Severity Scale For Diabetic retinopathy
Based on Wisconsin(WESDR) and ETDRS Classification
1. No Apparent Retinopathy
2. Mild nonproliferative – presence of microaneurysms
3. Moderate nonproliferative – Microaneurysms with intraretinal Haemorrhages or Venous beading
4. Severe nonproliferative -4:2:1 rule as per ETDRS
- If Hemorrhages of at least the magnitude of standard photograph 2A are present in all 4 quadrants, then by definition severe NPDR is present.
- If 2 quadrants or more have venous beading (VB) of the same magnitude or greater than standard photograph 6A, then by definition severe NPDR is present.
- If one or more quadrant has intraretinal microvascular abnormalities (IRMA) of the same magnitude or greater than standard photograph 8A, then by definition severe NPDR is present
5. Proliferative retinopathy It is characterized by neovascularization on or within one disc diameter the disc or neovascularization of the retina elsewhere ,
6. Advanced Diabetic Eye Disease There is neovascularization of the iris, neovascularization of the angle, neovascular glaucoma ,vitreous hemorrhage or tractional retinal detachment.
Newer Diagnostic modalities available
1. Optical coherence tomography
2. Fundus Fluorescein Angiography
OPTICAL COHERENCE TOMOGRAPHY CLASSIFICATION OF DIABETIC MACULAR OEDEMA
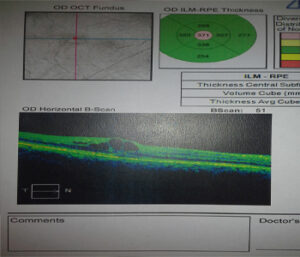
Optical coherence tomography (OCT) is a non-invasive, noncontact transpupillary imaging modality which utilizes light to image tissue using low coherence interferometry.
Advantages of OCT
A. OCT produces cross sectional images of the macula allowing objective evaluation of macular thickness
B. It allows evaluation of the vitreomacular interface.
Disadvantages of OCT
-Cost of the required equipment which limits its availability
-OCT findings may not correlate with vision and clinical findings in CSME
Clinically significant Macular Edema
1. Retinal thickening within 500 µm of the macular center
2. Hard exudates within 500 µm of the macular center with adjacent retinal thickening.
3. One or more disc diameters of retinal thickening, part of which is within one disc diameter of the macular center.
OPTICAL COHERENCE TOMOGRAPHY CLASSIFICATION OF DIABETIC MACULAR OEDEMA
Optical coherence tomography (OCT) is a non-invasive, noncontact transpupillary imaging modality which utilizes light to image tissue using low coherence interferometry.
Advantages of OCT
A. OCT produces cross sectional images of the macula allowing objective evaluation of macular thickness
B. It allows evaluation of the vitreomacular interface.
Disadvantages of OCT
-Cost of the required equipment which limits its availability
-OCT findings may not correlate with vision and clinical findings in CSME
Clinically significant Macular Edema
1. Retinal thickening within 500 µm of the macular center
2. Hard exudates within 500 µm of the macular center with adjacent retinal thickening.
3. One or more disc diameters of retinal thickening, part of which is within one disc diameter of the macular center.
OCT patterns of morphological macular changes associated with Diabetic Macular Edema(DME)
A. diffuse retinal thickening,
B. cystoid macular edema,
C. posterior hyaloidal traction,
D. serous retinal detachment
E. tractional retinal detachment.
Treatment for Diabetic retinopathy
1. Regular screening in all patients of diabetes to detect retinopathy
2. Pan Retinal Photocoagulation(PRP)
3. Macular Laser
4. Intravitreal injections
5. Vitreo-retinal surgeries
Screening for Diabetic Retinopathy
1. WHO?
Should be done by Ophthalmologist
2. HOW?
• With dilated pupils
• Direct and Indirect Ophthalmoscopy
• Sit Lamp Examination with 90DLens
3. WHAT to look for? • Visual acuity
• Severity of diabetic retinopathy
• Maculopathy
• PDR
• Other complications
4. WHAT to treat? • PDR
• MACULOPATHY